Urinary lithiasis
A more common disease in men
More commonly known as urinary calculi (stones), this disorder affects the upper part of the urinary tract. It concerns in priority men but women can also be affected.
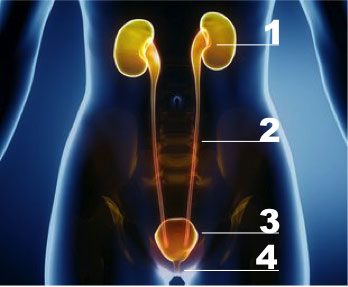
Urinary tract stones begin to form in a kidney and may be located in the entire urinary system, that is to say the kidney (1), the ureter (2), the bladder (3) and the urethra (4).
The most frequent stones are located at the level of the kidney and the ureter.They are discovered when patients get to emergency for a renal colic (back pain in the area between the ribs and hip, that spreads across the abdomen and sometimes extends to the genital area).
Apart from emergency situations, stones can be discovered during an imaging examination for back pains or urinary infections with a radiography, an echography or a scanner.
This medical treatment can be given intravenously or orally at home. It is recommended to filter ones' urine after renal colic to verify that the stones were eliminated. It also enables to determine the nature of the stones and avoid the formation of new ones.
• If the stone leads to a severe renal dysfunction, urine drainage is urgently required.
• If the pain is not relieved by the anti-inflammatory, a cathether is also put in place.
• Finally if the stone is superior to 7mm, it is better to put in place a catheter because of the low probability that the stone has not to descend alone.
If a catheter is put in place or if the stones require a surgical care,one of these 3 procedures is proposed according to the size and the location of the stones :
Extracorporeal shock wave lithotripsy
This procedure is aimed at breaking up kidney stones by sound waves produced by a lithotriptorla. Multiple fragments are obtained and they will be eliminated through the natural routes.
This technique is carried out under local or general anesthesia in one or several sequences.
Nevertheless this efficient technique shows some limits. Visualization of the stone can be done through a live radiographic test or ultrasound ; but in case the stone is difficult to locate the gesture is not efficient or cannot be made. For instance, morbid obesity is a factor that reduces the effectiveness of shock waves and the ability to spot stones.
A too large size of stone (greater than 1.5 cm) reduces the effectiveness of the procedure and may increase the number of lithotripsy sessions and cause renal colic.
A lower renal location makes it difficult to eliminate stones debris even if they are small and fragmented.
Finally, it is contraindicated to perform a lithotripsy for patients taking anticoagulants (treatment that is becoming more and more common).
Lenght of the stay
2 to 3 days
Duration of the surgery
Between 80 and 90 minutes
Surgery follow-up
Between D+7 and D+10
Flexible and rigid ureteroscopy
These two surgical techniques are performed under general anesthesia in the operating room and are part of so-called endo-urological techniques. It consists in introducing a miniaturized camera by the natural route up to the area of the stone. The latter is fragmented thanks to pneumatic lithotripters or laser waves and removed with the help of very small clips.
Rigid ureteroscopy is used for ureteral stones whereas flexible ureteroscopy is used for intra renal stones.
Big size stones (greather than 1.5 cm) sometimes require several interventions to fragment and destroy the entire stone.
The generalization of this technique and its attractiveness have made it more efficient and more predictable than lithotripsy but it remains a technique using a fragile and expensive technology. At the end of the procedure, it is often necessary to insert a probe in the ureter because of the inflammation caused by the passage of endoscopic instruments and the fragments of stones. It can also ease the flow of the remaining fragments. This probe will be removed afterwards during a consultation.
Percutaneous nephrolithotomy
For big size stones (in particular Staghorn stones that are large branching stones that fill part of all of the renal pelvis), the reference procedure is percutaneous surgery.
Percutaneous nephrolithotomy is a procedure used to remove kidney stones from the body when they can’t pass on their own. A scope is inserted through a small incision in your back to remove the kidney stones. The latter is fragmented thanks to pneumatic lithotripters and fragments are extracted one by one. A drainage by a probe is put in place at the end of the intervention in the puncture orifice. Then the probe is removed and healing is definitive after a few days.
This efficient procedure for large volume stones is an invasive technique that can cause hemorrhagic complications, fistulas or colic or pleural injury.
Nevertheless the evolution of the material and imaging techniques has reduced these risks. Consequently this procedure is more and more followed by specialized departments.
Combined treatments
The three previously explained techniques are complementary and enable to put in place synergies to improve the treatment efficiency.
In addition, these three techniques require specific equipment and experience accessible in our Urology Department.
Open or laparoscopic surgery
In some specific cases, for particular locations, exceptional sizes or if there is a malformation (junction syndrome for example), it is sometimes recommended to approach the kidney or the excretory ways, including the bladder by performing an intervention by conventional open surgery or laparoscopic surgery or robot-assisted surgery.
Dietary and hygienic laws
The simple stones treatment is not sufficient in the lithiasis disease care.
Indeed, it is important to try to determine the origin of the formation of the stone.
This is feasible thanks to the spectrophotometric analysis of the stone and a simple phosphocalcic test.
Some simple rules of hygiene can prevent a recurrence of this phenomenon in the majority of cases. Abundant hydration of at least 2 liters per day to increase urination is necessary. A balanced diet neither too rich in protein nor too rich in salt is also a good precaution to avoid recurrence.
Finally, for the most complicated cases, a complete aetiological assessment should be carried out with the help of a nephrologist.