Kidney cancer
Men are more affected than women
Kidney cancer is the 9th cancer in France in terms of number of cases (11 000 new cases each year). It’s the most deadly cancer.
Men are usually more affected than women by kidney cancer. More genrally speaking, this cancer usually affects adults in their 60s or 70s.
Risk factors for kidney cancer are the following ones: renal failure, smoking, obesity, high blood pressure and family history in kidney cancer.
You may have one or more of these symptoms: blood in your urine, low-back pain, a lump in your side or abdomen, general signs (fever, fatigue, weight loss) or abnormal blood tests.
In two-thirds of cases it is fortuitously discovered during a diagnostic imaging test.
Indeed there are many types of benign kidney tumors as well as cysts that are often benign.
Your urologist usually prescribes a radiological examination for clarification (Uroscanner). For some particular cases some additional radiological examinations can be recommended, such as UroMRI or a contrast study. The radiological assessment is key as it gives a good overview of the lesion nature, size, location and stage. Thus it enables to make a choice between a simple watch for benign or small tumors and a specific treatment for other patients. In certain cases a biopsy of the tumor is necessary for histological confirmation (celle studies).
The first one is to remove all the cancerous tissues.
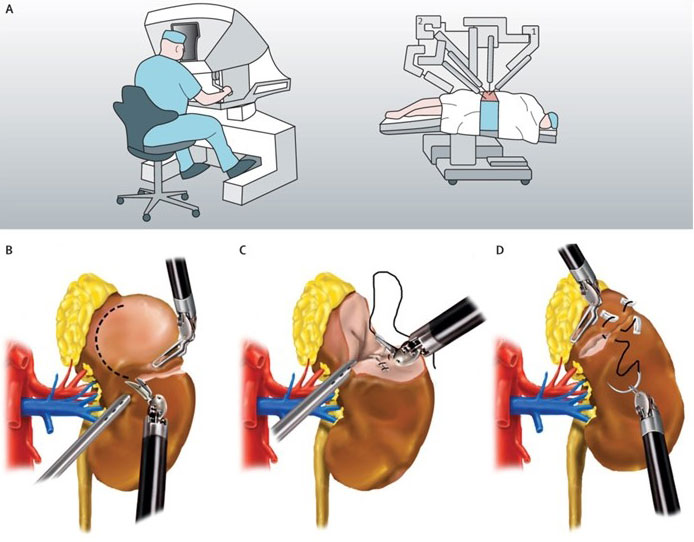
The second one is to preserve the kidney functioning (as it is technically feasible)thanks to a partial nephrectomy (partial removal of the kidney). The surgical indication depends on the tumor size and location as well as the invasion or not of neighbouring organs. It can be performed by open way (horizontal incision below the ribs or more lateral) or coelioscopic way with robotic assistance which decreases surgery pains and shortens the recovery time.
The surgery process
The surgery is performed under general anaesthesia.
The belly is inflated with carbon dioxide, providing a some work space for the surgeon.
5 to 7 small incisions are made, enabling to insert the camera and the mini-instruments necessary for the intervention.
A few meters by the operating table, the surgeon operates from a console and controls the robot movements with the 3D vision of the camera. The gestures are more accurate thanks to the robotic assistance.
A surgical assistant and a block nurse are constantly present in the surgery room and they actively participate to the surgery procedure.
Lenght of the stay
3 to 10 days
(average of 6 days)
Surgery follow-up
After 4 to 6 weeks
Once the tumor is removed, it is analyzed through an anatomopathological study (analysis of the tissues). The way you will be followed-up depends on the outcomes of this study.
Patient care and follow-up for kidney cancer involves lots of different actors. We work closely with other departments of Colmar Civilian Hospitals such as the radiology, oncology and anatomopathology departments in order to achieve the best patient care quality possible and to make you benefit from the latest technological and scientific progress.
Is there an alternative to standard surgery ?
Yes,
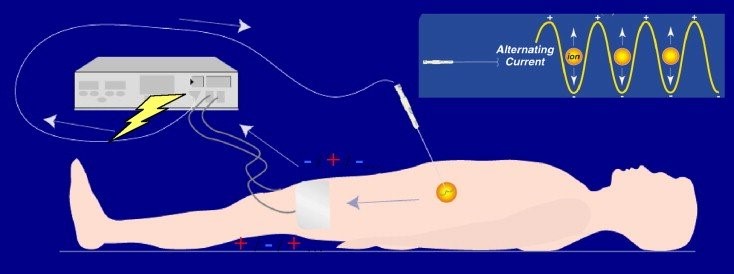
Colmar Civilian Hospitals have a team of interventional radiologists and a technical platform that enable to propose radiofrequency ablation (treatment that burns the tissues thanks to a needle placed through the skin).
This mini-invasive technique is quite recent and is currently under evaluation but its efficiency is probably inferior to the surgery. That is why it is reserved for patients with strong anesthetic risks.